A radiological bomb, also called a “dirty bomb”, is a conventional bomb, surrounded by radioactive materials intended to be spread as dust during the explosion.
The explosion of a dirty bomb therefore results in heat phenomena (burns), mechanical phenomena (wounds), equivalent to those of a conventional bomb, but also in radiological phenomena intended to contaminate a geographical area and the people present, by direct radiation (first effect) and the ingestion and inhalation of radioactive materials (second effect). It is therefore part of the “Improvised Explosive Devices (IED [1])” in the same way as those loaded with chemical or biological products (CBRN). We have already discussed in this blog the meaning of the “e (explosive)” added to NRBC to form NRBCe.
De quoi est-il question ?
The development of an atomic bomb is extremely difficult and can only be done at a state level.
On the other hand, if the fabrication of an explosive is not very difficult, adding radioactive elements to it can prove to be a little more complicated: it is necessary to find a radioactive source and to know how to manipulate it…. This type of explosive could therefore be used by a terrorist organization of a certain scientific level, such as the Aum sect, which in 1995 was able to organize the Sarin gas attacks in the Tokyo subway. [2] A dirty bomb will serve above all to provoke fear: fear of the unknown, of the invisible, of the atom.
The explosion of such a device cannot cause a destructive shock wave as in the case of an atomic bomb, since there is no fission or fusion reaction. On the other hand, if it can cause injuries and burns as in any explosion, it is accompanied by a dispersion of radioactive elements (generally nuclear waste from laboratories or hospitals…), such as cobalt 60, strontium 90, cesium 137, iridium 192, polonium 210, radium 226, plutonium 238, americium 241, californium 252…
Radioactive contamination
Irradiation, during which the object or being is subjected to ionizing radiation, should not be confused with contamination by radioactive dust that can be deposited on surfaces, including the body surfaces of people in the vicinity.
In low concentrations, these elements are generally not able to cause acute radiation syndromes followed by death as in the case of an atomic bomb. On the other hand, it is the distribution of radioactive dust that is of concern, because it can penetrate the human body and produce deleterious effects. As a result, the number of potential victims is much higher than the number of people physically affected by the explosion.
Not to mention the panic effects as well as the indirect economic effects of decontamination actions aimed at eliminating long-lasting radioactive contamination, on critical infrastructures for example.
External contamination can enter the body and cause long-term consequences, usually cancer. In addition, it can cause secondary contamination, especially of first aiders and hospital workers.
Contamination can spread in the atmosphere depending on humidity and weather conditions: heavier particles fall to the ground near the point of emission while lighter ones can diffuse as aerosols. Contaminated soil and water cause contamination of the food chain: animals drink the water from rivers, cattle eat the grass, humans eat the animals, etc.
Some patients can be expected to suffer blast injuries. They will have mechanical trauma from metal fragments of the bomb as well as burns. Although external irradiation by ionizing radiation cannot be ruled out, the risk of developing an acute illness is very low. The external contamination deposited on the body can then lead to the incorporation of the radionuclide(s) into the body. When isotopes are incorporated into an individual, they concentrate in certain organs such as the bones, thyroid, digestive tract, liver and central nervous system and promote the development of cancers through DNA damage.
Let’s not forget that some radioactive products present, in addition to their radiotoxicity, a chemical toxicity that can constitute the most important risk, as is the case for actinides, uranium or plutonium.
Emergency medical measures
In a 2018 publication, Rump et al [3]. share their position on emergency response to a dirty bomb explosion.
Because ionizing radiation is not visible, the local dose rate must be assessed using radiation measurement and detection equipment. In the case of high radiation dose levels, victims should be quickly evacuated from the area. Those who are only externally irradiated (usually far away from the explosion site) do not pose any particular danger to rescuers or hospital personnel.
Those that are externally contaminated with radioactive materials (e.g., contaminated dust from the detonation), may endanger their surroundings through cross-contamination. Members of the rescue teams must protect themselves, in particular by wearing protective clothing, respiratory protection (particle filter mask that also protects the eyes) and gloves. Ouvry’s polycombi [4]® is particularly well suited for first aid personnel working in this environment. In the same vein, Ouvry has developed a suit specially adapted to professionals working in nuclear power plants: the Polynuc [5]®
Rump et al. focus on the so-called “combined” type of injuries = mechanical/thermal injury + radiation and/or radioactive contamination). It should be noted that mechanical injuries may result in an immediate life-threatening situation (e.g., tension pneumothorax, massive intra-abdominal hemorrhage…), whereas the acute consequences of radiation action develop with a latency ranging from days to weeks. Even prodromal symptoms such as nausea or vomiting may not appear for several hours.
The same is true for the incorporation of radionuclides, followed by long-term internal irradiation, which will probably only cause health effects in the long term.
As in any medical emergency, the principle “Treat first what kills first” applies here. Preservation of vital functions is always the priority. Thus, the initial triage should be performed according to the general rules of trauma medicine. The application of specific triage systems for radiological accidents does not make sense at this very early stage, but should be reserved for the retriage of patients at a later stage.
Victims without serious injuries and no indication of urgent medical action should first be fully decontaminated by undressing and body flushing. Before starting any further medical monitoring or treatment, decontamination should be verified by radiation measurements.
Decision-making is more complex in the case of severely physically injured patients, as the urgency of surgical treatment must be weighed against the transfer of radioactive contamination to emergency vehicles, emergency rooms and operating rooms.
In the case of a patient with an urgent life-threatening indication for surgery (e.g., massive intra-abdominal hemorrhage), at least a provisional decontamination should be performed by undressing the victim before transport. This simple and rapid procedure should remove a large part of the radioactive contamination that has settled on the clothing (70-80%).
When radionuclides are incorporated, they are distributed in the body and deposited in different tissues and organs, depending on their chemical nature. Their natural elimination from the body is variable and occurs by the same excretion mechanisms as for stable (non-radioactive) chemical entities, as well as by radioactive decay. The effective half-life, depending on the two processes, varies from a few days (iodine-131: 7-8 days) to a few months (cesium-137: 109 days) and to decades (plutonium-239: 50 years).
The radioactive decay of radionuclides leads to a prolonged and, in part, lasting irradiation of the body from within. Except in rare cases, experience shows that the absorbed doses in a short period of time are well below the threshold of an acute radiation sickness. However, continuous irradiation increases the risk of random health effects, such as the future development of tumors and other pathologies.
Decontamination actions
External decontamination
The decontamination of materials, structures and people’s skin will be done by well known techniques according to the usual protocols of professionals.
The DECPOL RAD [6]® radiological decontamination wipe from Ouvry is particularly well adapted to this situation: composed of a 100% viscose non-woven element impregnated with a RADECOM® degreasing solution, it decontaminates surfaces by “transferring” radiological particles, without over-contaminating by spreading or re-depositing. The liquid that impregnates the wipe does not generate a liquid surplus. The wipe is effective on all types of surfaces as well as on the skin.
The decontamination of the skin is intended to prevent the transfer of radioactive particles that have been deposited there, inside the body: this is called “incorporation”.
Internal decontamination or decorporation
How can radionuclides be extracted from the organism into which they have entered?
The products
Internal decontamination allows the radionuclides in the body to be reduced or even eliminated. This is called “decorporation”.
First, Prussian Blue or DI Blue (DI: internal decontamination) is a ferrocyanide, distributed under the name of Radiogardase.
This large chelating molecule absorbs cesium 137 and thallium by trapping them in a definitive way. Not being absorbed in the blood at the level of the digestive tract, it is eliminated with its radionuclide in the stools then colored in dark blue.
Ca-DTPA (sometimes Zn-DTPA) (diethylenetriaminepentaacetic acid) exchanges the less firmly bound calcium ion for many metal radionuclides, including plutonium-239 and americium-241, and accelerates their renal excretion.
Other decorporants exist, each removing different types of radionuclides.
Once the radionuclide has been identified, the selection of the correct antidote is usually not a problem. However, there is no consensus on when to start treatment.
When should treatment be started?
According to the “precautionary approach”, one should wait for the results of internal dosimetry and only start decorporation treatment if a relevant committed effective dose has been confirmed (> 20 mSv or > 200 mSv, depending on the standard set). This approach emphasizes that exposing a patient to the potential side effects of a drug is not justified until the actual need is clear. According to the “urgent approach”, it is prudent and advisable to begin decorporation treatment immediately, even if radionuclide incorporation is only suspected. Treatment should be discontinued when the results of internal dosimetry are available and it has been demonstrated that treatment is not relevant.
Simulation of the time course of radioactivity in the central compartment (blood and extracellular space) resulting from a wound contaminated with a highly soluble plutonium-239 compound shows that the activity increases rapidly until the end of the second day and then decreases to very low values after about 10 days (Fig. 1).
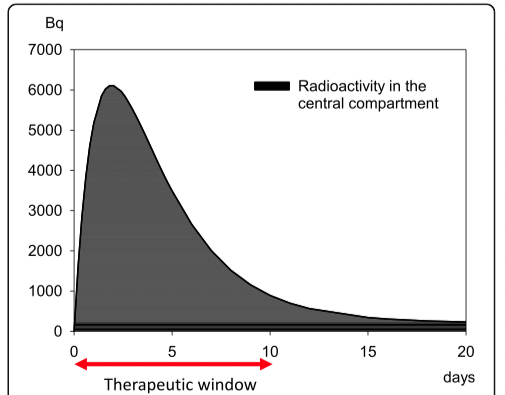
FIg. 1: Evolution of radioactivity in the central compartment (blood, extracellular space) following a wound contaminated with 37 kBq (1 μ Ci) of plutonium-239 as a soluble compound. The activity drops to low values after about 10 days. The decorporation agent Ca-DTPA is distributed primarily in the extracellular space, where it can bind plutonium.
The treatment must therefore begin within 10 days to be very effective: this is the “therapeutic window”.
At the same time, plutonium-239 is redistributed into “deep” compartments such as bone and liver. Ca-DTPA, the agent of choice for decorporation of plutonium-239, is distributed mainly in the extracellular space, where it can bind plutonium. Thus, there is a window of opportunity during the first 10 days after the incident to achieve high therapeutic efficacy, and even during this period, a delay in initiating treatment will be associated with decreased efficacy because the total amount of plutonium that can be rapidly removed decreases. Once plutonium has entered the “deep” compartments, it cannot be bound by Ca-DTPA in significant amounts.
Therapeutic efficacy can be increased by extending the duration of treatment. However, there is limited opportunity to compensate for a delay in initiation of therapy by extending the duration of treatment.
The maximum therapeutic efficacy and the consequences of a delay in the initiation of treatment depend on the radionuclide, the route of invasion and the physicochemical properties, in particular the solubility of the compounds involved. It is therefore not possible to give a precise time frame for the initiation of treatment by decorporation. Depending on the situation, it seems to be in a range from a few hours to several days.
The undesirable side effects of these drugs are known, but they seem to be relatively unimportant in short-term treatments, so the strategy of the “urgent approach” seems prudent and has been adopted at the Institute for Radiobiology of the Bundeswehr (to which the author of the article belongs). However, depending on the magnitude of the incident, this strategy may require a very large number of daily doses of antidotes and requires corresponding investments in preparedness by the responsible authorities.
Conclusions
Nuclear and radiological scenarios can be very different in nature and scale. In the case of a “dirty bomb” attack, patients with mechanical and thermal trauma are to be expected, in addition to a much larger number of victims who have potentially incorporated radionuclides. Therefore, in addition to appropriate technical and medical management at the incident site, a clear strategy for treating a large number of potentially internally contaminated patients is mandatory. The early initiation of treatment, even on the basis of a mere suspicion of radionuclide incorporation, according to the strategy of the “urgent approach”, seems to be medically sound but requires a demanding policy of antidote storage.
References
Rump A., B. Beker, S. Eder, A. Lamkowski, M. Abend, M. Port. Medical management of victims contaminated with radionuclides after a « dirty bom »attack, Military Medical Resarch (2018), 5, 2-10, https://doi.org/10.1186/s40779-018-0174-5 [7]
https://www.techno-science.net/glossaire-definition/Bombe-radiologique.html [8]
https://fr.wikipedia.org/wiki/Contamination_radioactive [9]
Autor: Prof. François Renaud